

.svg)
Why Defensible Documentation Is the Most Important Business Decision You Will Make in 2026




In an era of tightening payer scrutiny and rising audit activity, the practices that thrive will be the ones that treat documentation as a clinical and operational standard, not an afterthought. This blog breaks down what medical necessity really means, what "defensible" documentation looks like, and how the right workflows and technology can make excellence achievable every single day.
It isn’t a new technology, a new service line, or a new payer contract. It’s documentation and here’s why:
Every wound care practice in 2026 is navigating the same pressures. Reimbursement per visit has fallen due to the new pressure on skin substitutes. Greater efficiency, more patient visits, and diversified revenue streams are likely at the top of your agenda. In this environment, it is tempting to focus on big strategic moves like new service lines, new technology investments, and new referral relationships.
However, the single highest-return investment most wound care practices can make this year isn’t any of those things. It’s documentation. Not documentation as an administrative checkbox or something the billing team worries about after the fact. Documentation as a clinical discipline, an operational standard, and ultimately, the foundation on which sustainable wound care revenue is built.
“The most expensive documentation mistake in wound care is billing for a service that was performed correctly and was clinically appropriate for the patient but which cannot be defended because the notes don’t tell the story.”
The practices that understand this distinction, and build their workflows around it, will be more financially resilient and better positioned to grow in the years ahead. The ones that don’t will keep losing revenue to pre-auths, WiseR non-affirmations, claim denials, and recoupments that were all entirely preventable.
Documentation Is a Clinical Standard, not a Billing Concept
This is where most practices go wrong: they think of documentation as something that happens at the end of the clinical encounter, in service of getting paid. That framing gets it exactly backwards.
Medical necessity, the standard that governs whether a payer will reimburse a service, is not just a billing construct. It is a clinical standard that must be demonstrated in writing through every single encounter. The treatment provided must be appropriate for the patient’s condition, consistent with evidence-based standard of care and payor policies, and documented thoroughly enough that a reviewer who never met the patient can understand the clinical decision-making.
That last point deserves emphasis: document as if an auditor or claims analyst will read every note because, eventually, one might.
Medical necessity applies to everything you bill, not just advanced therapies. Every E&M visit requires documented justification for the level billed. Every debridement requires documentation of the clinical rationale. Every dressing selection requires documentation of the wound status that warranted it. And every advanced therapy whether it be CTP, PRP, or UltraMIST requires a documented clinical story that begins weeks before it is ever applied.
What “Defensible” Actually Looks Like
Defensible documentation isn’t a higher standard reserved for complex cases. It is the baseline standard for every note, every visit. In practice, that means documentation that meets four criteria:
1. Specific: Wound measurements, photos, tissue type, exudate level, and periwound condition captured at every visit, not selectively.
2. Sequential: A clear record of how the wound has changed over time and how the treatment plan has responded to those changes.
3. Justified: Documented evidence of why the previous approach was insufficient should precede every escalation in therapy.
4. Complete: The 'why' behind every clinical decision is in the note. This is not assumed, not implied, not reconstructed later.
When these four elements are consistently present, a note does more than satisfy a payer. It tells the clinical story of a patient’s care in a way that is both understandable and defensible.
Making Documentation Excellence Operationally Possible
Knowing what to document is only half the equation. The other half is making it operationally possible to do it consistently, at every visit, with every patient, regardless of how busy the day gets. This is where many well-intentioned practices fall short. The clinical team understands the standard; the workflow doesn’t support it.
The documentation habits that protect a practice are not complicated, but they require structure to be reliable:
1. Photograph wounds at every visit using standardized imaging. Wound photos are one of the most powerful documentation tools available and one of the most commonly missing elements in audited charts.
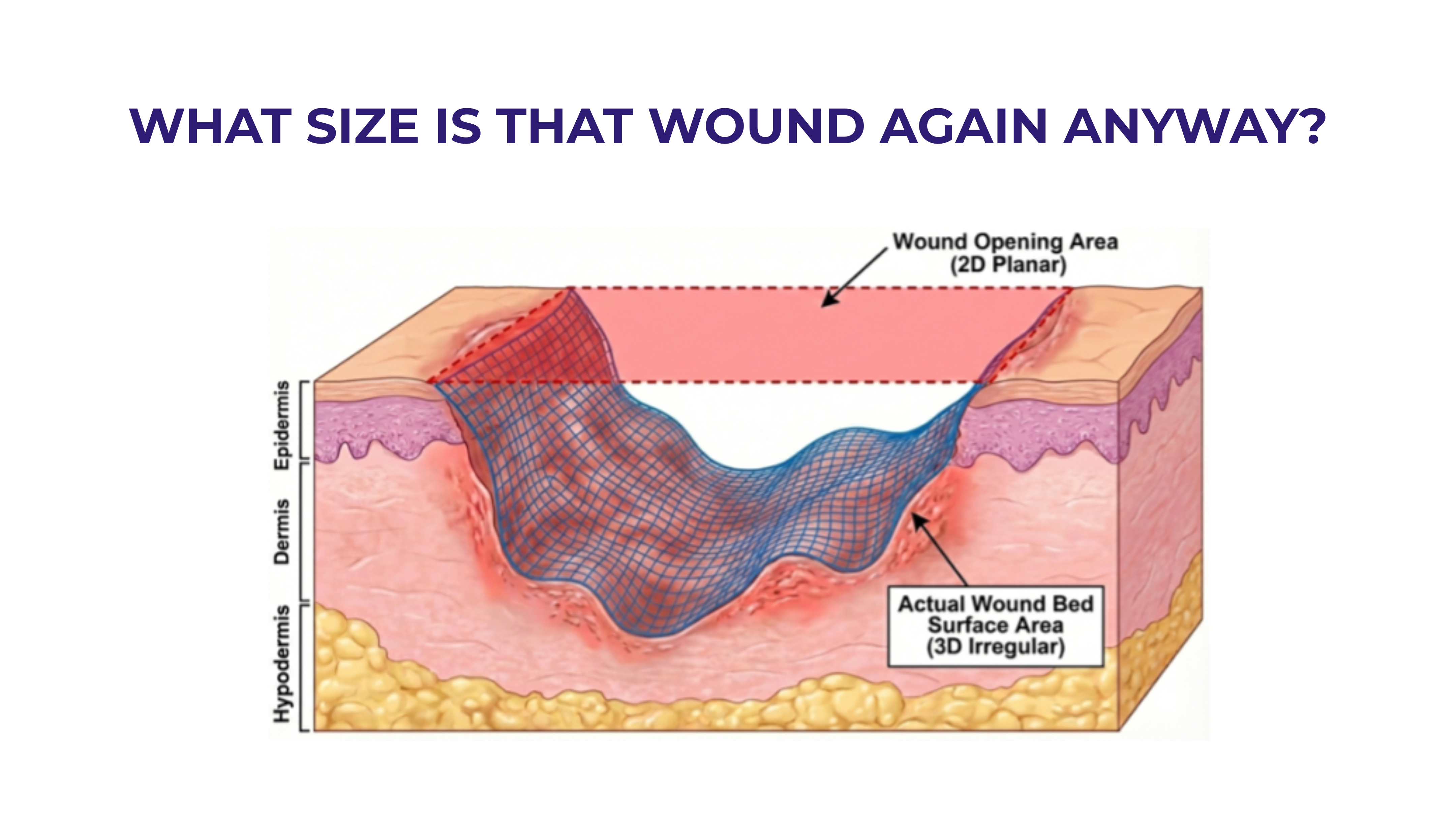
2. Capture objective measurements at every visit: length, width, depth, wound area in cm². This is the data that proves or disproves wound response over time.
3. Document the “why” alongside the “what.” Not just “applied CTP,” but “applied CTP due to documented failure to achieve 50% area reduction after 6 weeks of standard care.”
Technology That Supports Defensible Documentation
The right technology stack makes consistent, high-quality documentation achievable without adding burden to an already stretched clinical team. Three categories of tools deserve particular attention:
1. Wound Specific EHRs: Platforms like Medipyxis, Net Health, and Intellicure build evidence-based standard of care prompts and compliance checks directly into the clinical workflow, so documentation gaps are caught in real time, not during a prior auth review or an audit.
2. Wound Imaging Tools: Tools like Swift automate measurement, track wound area reduction over time, and generate compliance dashboards turning photography from an afterthought into a clinical data asset.
3. AI Clinical Note Review: Solutions like Venture OneView catch documentation gaps before claims are submitted not after they are denied. This is the step that converts good intentions into protected revenue.
The Pre-Billing Review: Make It Non-Negotiable
Before any advanced therapy is applied, the clinical note should be reviewed against the medical necessity criteria for that specific therapy. This is not an administrative burden; it is the step that protects your practice from a costly mistake. Think of it as a final quality check: if the notes can’t defend the application, the product should not be used.
Documentation Is a Competitive Advantage
Most wound care practices think about documentation defensively - as a way to avoid audits, denials, and recoupments. That’s a valid reason to prioritize it. But the most forward-thinking practices understand that documentation excellence is also an offensive strategy.
Practices that document well accumulate something that practices that don’t never will: a longitudinal, data-rich record of their clinical outcomes. That data is a business asset. It supports quality reporting and strengthens payer relationships. It differentiates the practice in a competitive referral market. And increasingly, as value-based care models expand into wound care, it will be the currency through which reimbursement is determined.
The revenue cycle benefit is equally concrete: fewer denials mean lower administrative overhead, faster payment cycles, and less revenue leakage. Every claim that doesn’t get denied is a claim that doesn’t require a rework team. Every audit that results in no findings is one that doesn’t cost the practice weeks of staff time and legal exposure.
The practices that will lead wound care in 2026 and beyond are the ones building documentation into their operational DNA right now. The investment is real, but so is the return: in protected revenue, in clinical credibility, and in a practice that is built to last


Categories


Navigating WISeR: What Wound Care Providers Need to Know and How Venture Medical Can Help
The WISeR Model is here, and it's changing the way wound care providers submit and manage their Medicare claims. Learn what WISeR means for your practice, why accurate documentation is more critical than ever, and how Venture Medical is working hand-in-hand with providers to navigate the process with confidence.

How Venture Medical Is Helping Providers Build Practices That Last
Venture Medical remains committed to being a long-term partner to providers by giving them the strategies and tools they need to build sustainable, resilient practices for the long haul.Venture Medical's ongoing 2026 webinar series is focused on helping wound care providers build practices that can absorb disruption rather than react to it. Learn more about this webinar series and watch the recaps of the sessions you might have missed.





Missoula, Montana