

.svg)
What size is that wound again anyway?



CMS's 2026 skin sub wastage policy allows providers to bill onlyfor units "administered," not "discarded." Cue the nightmare scenario: measuring grafts centimeter by centimeter to exactly fit the "wound area."
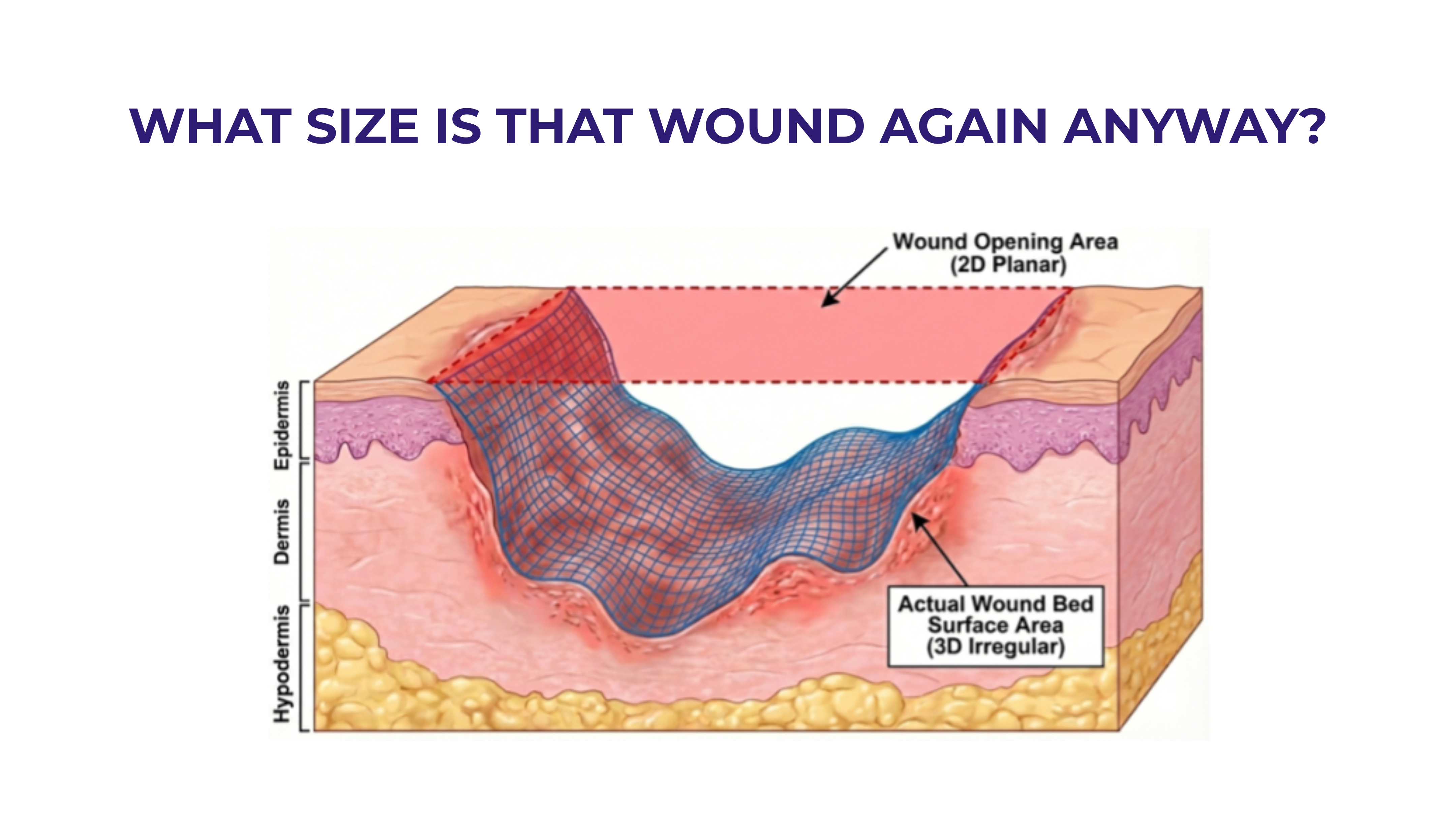
But here's the problem—what even is the wound area?
As several well-known clinicians have observed, there are two very different "areas" at play. One put it this way: “It’s a little like painting a room, do you want to just paint the ceiling or do you want to paint the walls too?”
In most wounds there is the 2D wound opening area at skin level—historically estimated as length × width, now calculable with modern AI tools. Then there is the actual 3D surface area of the wound bed. For skin substitutes to be administered as intended as a protective covering in compliance with FDA rules, it's the actual 3D surface that matters. That is what the graft contacts.
The gap between these two measurements is larger than most people realize.
Using simple geometric models: → Shallow wounds: up to 20% difference → Moderate depth: up to 100% → Deep wounds: 400% or even more
Calculating the true wound bed surface area requires full 3D surface mapping—not something you get from L × W × D. @ShaunCarpenter has proposed a clever drape-based estimation technique, but however you approach it, the wound bed surface you need to cover is likely substantially larger than the 2D opening suggests.
Now add to this the requirement for edge overlap. Many skin subs need to extend beyond wound margins to cover the wound edges and for fixation according to the manufacturer’s instructions for use. Even a conservative 0.5 cm overlap adds significantly—for smaller wounds, potentially an additional 100-200% of the wound opening area. For large wounds, it is still 25% or more.
So, what size skin sub actually needs to be "administered"?
The best available answer: highly variable, often substantially larger than L × W, and dependent on depth, geometry, and margin requirements that vary with every unique wound. This is way more complicated than adding up centimeter by centimeter to get some ideal “perfect fit.”
For now, the best measurement tool remains the clinician at the bedside—eyes, hands, and clinical judgment, carefully documented (with wound images) to explain why a particular size of graft was chosen.


Categories



Navigating WISeR: What Wound Care Providers Need to Know and How Venture Medical Can Help
The WISeR Model is here, and it's changing the way wound care providers submit and manage their Medicare claims. Learn what WISeR means for your practice, why accurate documentation is more critical than ever, and how Venture Medical is working hand-in-hand with providers to navigate the process with confidence.

How Venture Medical Is Helping Providers Build Practices That Last
Venture Medical remains committed to being a long-term partner to providers by giving them the strategies and tools they need to build sustainable, resilient practices for the long haul.Venture Medical's ongoing 2026 webinar series is focused on helping wound care providers build practices that can absorb disruption rather than react to it. Learn more about this webinar series and watch the recaps of the sessions you might have missed.


Why Defensible Documentation Is the Most Important Business Decision You Will Make in 2026
In an era of tightening payer scrutiny and rising audit activity, the practices that thrive will be the ones that treat documentation as a clinical and operational standard, not an afterthought. This blog breaks down what medical necessity really means, what "defensible" documentation looks like, and how the right workflows and technology can make excellence achievable every single day.



Missoula, Montana